
Several years ago, I firmly believed that red dates (Hongzao) and Ejiao (Donkey-hide gelatin) could not nourish the blood, as nutrition teachers claimed that red dates have low iron content and that the absorption rate of plant-based iron is poor. They suggested consuming iron-rich foods like pig liver or duck blood instead, and dismissed the so-called effective components in Ejiao—donkey skin—as inferior protein.
However, I later realized that Charlie Munger’s saying, “A man with a hammer sees everything as a nail,” could not be more accurate.
Because in the past, including many nutritionists today, when discussing anemia, they often default to iron deficiency anemia without understanding the types of anemia or knowing how to apply more effective blood-nourishing methods than iron supplements.
Moreover, iron supplementation can be ineffective or even harmful for certain types of anemia, while using red dates, Ejiao, or nutrients other than iron can have excellent therapeutic effects.
Given that many people have recently left messages on the public account wanting to understand topics related to “anemia,” “blood nourishment,” and “iron supplementation,” I have compiled this article to help you “treat the symptoms appropriately.”
1
Are you anemic?
Red blood cells are common blood cells, with adults having between 3.5 to 5.5 million red blood cells per microliter of blood.
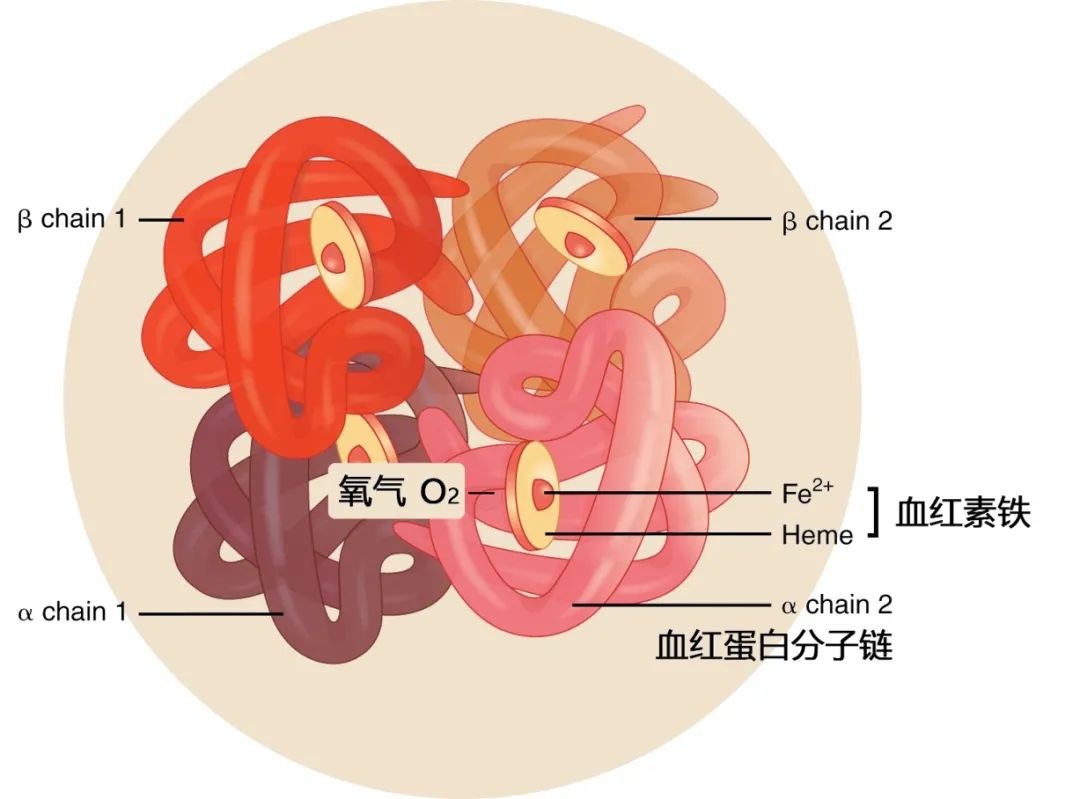
97% of the dry weight of red blood cells is hemoglobin, a protein that contains iron and is responsible for transporting oxygen (each gram of hemoglobin can bind 1.34 milliliters of oxygen).
Anemia, in a vivid sense, is somewhat like altitude sickness; it essentially results from a lack of sufficient red blood cells (hemoglobin) to deliver oxygen to tissues and organs, which can make a person feel weak.
Many health check items include a “complete blood count”; when hemoglobin concentration falls below 110g/L (for females) or 120g/L (for males), anemia should be considered.
The following are various manifestations of anemia (cellular hypoxia).
Reproductive system: decreased, increased, or irregular menstrual cycles
Digestive system: loss of appetite, abdominal discomfort, constipation, or diarrhea
Immune system: increased susceptibility to infections, decreased immunity
Endocrine system: affects adrenal and thyroid function
Neuromuscular system: fatigue, weakness, headaches, dizziness, tinnitus, difficulty concentrating
Respiratory and circulatory system: shortness of breath, rapid breathing, increased heart rate
Skin and mucous membranes: pallor or slight yellowness
2
What types of anemia are there?
The occurrence of anemia is mainly related to decreased red blood cell production and increased red blood cell destruction.
I. Deficiency or reduction of hematopoietic stem cell function
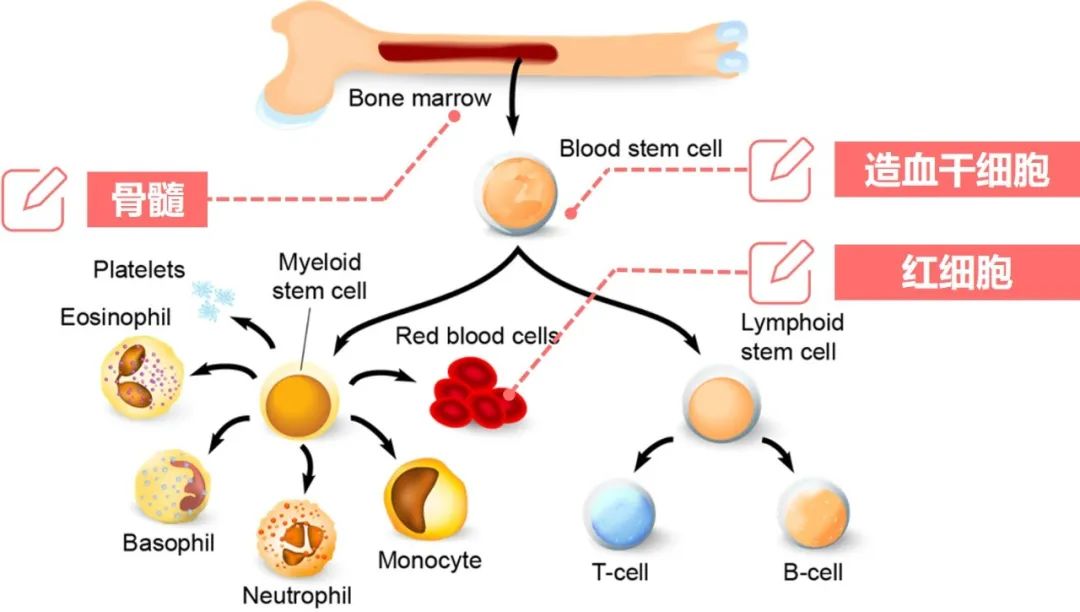
Red blood cells primarily originate from hematopoietic stem cells in the bone marrow. When the function of hematopoietic stem cells is lost or their number decreases, aplastic anemia can occur, which is characterized by decreased red blood cell production.
Common causes of aplastic anemia include bone marrow diseases, autoimmune diseases (such as systemic lupus erythematosus), undergoing radiotherapy or chemotherapy, using certain medications (such as chloramphenicol and drugs for rheumatoid arthritis), exposure to toxic chemicals (such as gasoline, pesticides, or insecticides), and infections from certain viruses (such as HIV, EB virus, parvovirus B19, or cytomegalovirus).
Individuals with this type of anemia often exhibit a decrease in red blood cell count along with a decrease in white blood cells and platelets.
II. Abnormal hematopoietic regulatory factors
The differentiation, development, proliferation, and maturation of hematopoietic stem cells are regulated by many environmental factors. Abnormal environmental factors can lead to hematopoietic dysfunction.
For example, renal anemia is caused by insufficient erythropoietin, a hormone also known as erythropoiesis-stimulating factor, which is normally secreted by the kidneys. When kidney function is impaired, erythropoietin secretion decreases.
In other words, when patients with renal failure develop anemia, the first consideration should be the use of erythropoietin rather than blindly supplementing iron (which can be used in conjunction if necessary).
Testosterone is also a hematopoietic regulatory factor. The reason men are less likely to be anemic than women is not only due to lower iron loss but also related to higher testosterone levels. Therefore, the saying that “nine out of ten women are anemic” may be exaggerated, but it is not without reason.
Other hematopoietic regulatory factors include tumor necrosis factor, interferon, and hepcidin, which can be upregulated or downregulated in various chronic inflammatory diseases, thus affecting the function of hematopoietic stem cells.
III. Insufficient hematopoietic materials
Hematopoietic materials include iron, vitamin B6, vitamin B12, and folic acid; a deficiency of any of these nutrients can lead to anemia.
Iron deficiency anemia is the most well-known type of anemia, characterized by small red blood cell volume and low hemoglobin content, classified as microcytic hypochromic anemia.
Determining whether iron deficiency anemia exists is straightforward; blood tests for serum ferritin, serum transferrin receptor, and free erythrocyte protoporphyrin can be conducted.
Serum ferritin reflects the body’s iron storage and is the most reliable indicator for diagnosing latent iron deficiency. A value below 15μg/L indicates depleted iron stores, while values exceeding 150μg/L (for females) or 200μg/L (for males) indicate excessive iron load. It is important to note that ferritin can increase in inflammatory states such as infections or liver cancer, which does not indicate iron overload.
Serum transferrin receptor reflects the number of receptors in immature red blood cells and the level of erythropoiesis. This indicator is not affected by infections or inflammation and can accurately predict iron nutritional status. The normal value for serum transferrin receptor is 0.9–2.3mg/L, and in iron deficiency anemia, this value is three times higher than normal.
Iron binds with protoporphyrin to form heme; if iron is insufficient, the concentration of free erythrocyte protoporphyrin will increase. The World Health Organization recommends using this indicator to assess the prevalence of iron deficiency in populations. When the concentration of free erythrocyte protoporphyrin exceeds 0.9μmol/L or protoporphyrin concentration exceeds 0.96μmol/L, or the ratio of the former to hemoglobin exceeds 4.5μg/g, it can be diagnosed as iron deficiency anemia.
Another common type of nutritional anemia is deficiency of vitamin B12 and folic acid, which is characterized by enlarged red blood cell volume and underdevelopment, hence also known as megaloblastic anemia.
Vitamin B6 is another hematopoietic material; its deficiency can lead to decreased enzyme activity that helps in heme production, preventing red blood cells from utilizing iron. This type of anemia is essentially sideroblastic anemia (related to genetic factors), where iron supplementation is ineffective or even harmful, but high doses of vitamin B6 can activate the missing enzymes, effectively treating anemia (vitamin B6 can also improve other types of anemia).
Finally, the aforementioned types of nutritional anemia all exhibit an increase in the red blood cell distribution width (RDW), indicating variability in the size of red blood cells produced by hematopoietic stem cells. In other words, an increased RDW suggests a lack of hematopoietic materials.
IV. Hemolytic anemia
Hemolytic anemia results from intrinsic defects in red blood cells and external factors (the environment in which red blood cells survive), characterized by a shortened lifespan of red blood cells, leading to the production of large amounts of bilirubin after their death. Depending on severity, it can lead to jaundice, gallstones, splenomegaly, abnormal urine color, thrombosis, and renal failure.
The so-called intrinsic defects in red blood cells generally refer to hereditary diseases, such as hereditary spherocytosis and elliptocytosis related to red blood cell membrane defects, glucose-6-phosphate dehydrogenase deficiency (favism), and pyruvate kinase deficiency related to red blood cell enzyme defects, as well as thalassemia (hemoglobin synthesis disorder) and sickle cell disease related to abnormalities in hemoglobin structure or function.
External factors include infections, toxins, oxidative stress, and autoimmune factors, which can also lead to the rupture and death of red blood cells, triggering hemolytic anemia.
This type of anemia requires tests for reticulocyte count, liver and kidney function, and urinalysis, as well as special tests such as red blood cell osmotic fragility test, glucose-6-phosphate dehydrogenase activity, direct Coombs test, snake venom factor hemolysis test, hemoglobin electrophoresis, and genetic testing for differential diagnosis.
Reticulocytes: immature red blood cells; a decrease is seen in aplastic anemia, while an increase is observed in iron deficiency anemia, megaloblastic anemia, and hemolytic anemia, with the most significant increase in hemolytic anemia (greater than 10%).
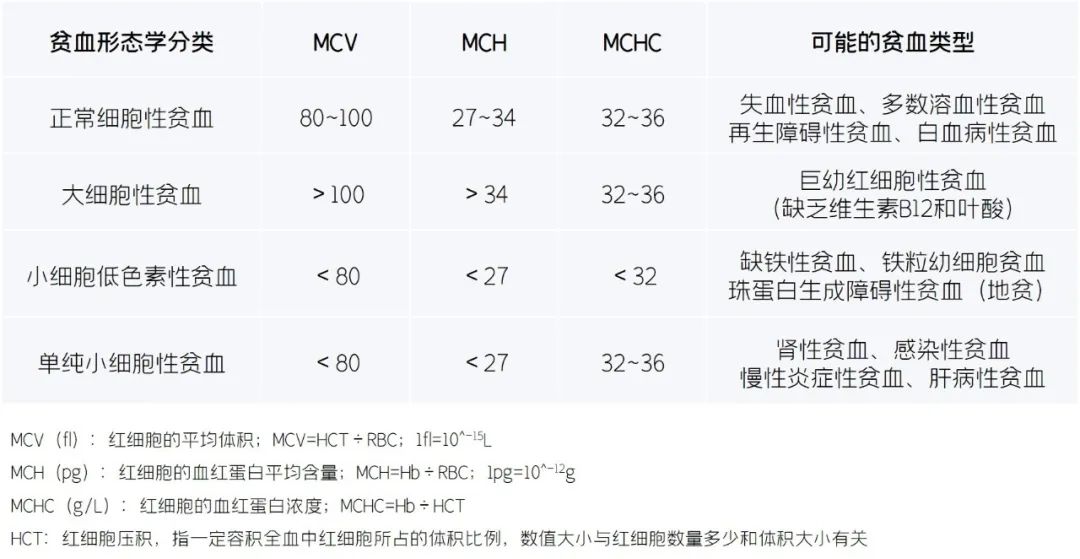
V. Morphological classification of anemia
The following table classifies different types of anemia based on red blood cell size and hemoglobin content.
3
Can iron supplementation treat anemia?
Although anemia is a disease, it often arises as a symptom secondary to other causes. Therefore, only by treating the upstream diseases that cause anemia can the condition be fundamentally corrected.
Taking the most common iron deficiency anemia as an example, insufficient intake of red meat and blood products can indeed lead to anemia, and iron supplementation can treat this type of anemia.
However, many people overlook the causes of poor iron absorption, such as gastrointestinal diseases.
Insufficient gastric acid is quite common; individuals with this condition may find that simple iron supplementation is ineffective (or even completely useless), and they need to add betaine hydrochloride or vitamin C to promote iron absorption. I recommend using glycine chelated iron, which is less irritating to the gastrointestinal tract and has a higher absorption rate, rather than cheap ferrous sulfate, which has significant gastrointestinal side effects.
Additionally, gastrointestinal ulcers can lead to hidden bleeding, and iron supplementation may increase gastric discomfort; in such cases, nutrients like short peptides, carnosine zinc, melatonin, and carotenoids should be used to repair the mucosa first. Medications that inhibit gastric acid secretion, such as omeprazole, can aid in ulcer healing but further reduce iron absorption.
It is also important to note that iron supplementation may be harmful for thalassemia and sideroblastic anemia, but the latter can easily be confused with iron deficiency anemia as both present as microcytic hypochromic anemia, so care must be taken not to supplement iron in patients with iron overload anemia.
4
Is iron supplementation during pregnancy scientifically justified?
There is no doubt that the demand for iron increases during pregnancy, but the appropriate dosage of iron supplementation varies from person to person.
In China, there are so-called comprehensive vitamin and mineral products designed for pregnant women, with each tablet containing up to 60mg of iron, but this dosage is unnecessary and should not be used, as studies have found that pre-pregnancy iron supplementation is associated with a 57% increased risk of gestational diabetes, which can be harmful to those who are not iron deficient.
My recommendation is to use low-dose iron combined with more active vitamin B6 (pyridoxal-5-phosphate), as vitamin B6 not only treats iron-refractory pregnancy anemia [1] but also improves morning sickness and gestational diabetes.
High-quality comprehensive vitamin and mineral products for pregnancy should contain appropriate amounts of highly absorbable organic iron and should not contain excessive calcium (as it competes with iron for absorption), while also adding sufficient active folic acid, vitamin B12, and vitamin B6.
5
Can eating red dates nourish the blood?
Some nutritionists claim that using red dates to nourish the blood is merely a connection based on the color “red,” as red dates have low iron content and their blood-nourishing effect is far inferior to that of pig liver or other animal products.
While it is true that red dates are not very effective for iron supplementation, it is scientifically inaccurate to say that they have no blood-nourishing effect.
After all, what evidence supports this claim? I found that consuming jujube fruit or its extracts can improve anemia.
An experimental study involving 31 primary school students found that consuming jujube fruit daily for two months increased the hemoglobin levels and hematocrit of the subjects [2].
Research has also shown that jujube extract not only contains a large amount of cyclic adenosine monophosphate but can also induce the synthesis of erythropoietin [3], both of which can stimulate hematopoietic stem cells in the bone marrow. Therefore, in populations with pregnancy-related anemia or chemotherapy-induced anemia, jujube extract has shown good therapeutic effects.
In 2017, Zhang et al. from the Obstetrics and Gynecology Department of Beijing Chaoyang Hospital recruited 120 anemic pregnant women for a clinical trial, which indicated that jujube extract could significantly improve pregnancy-related anemia [4].

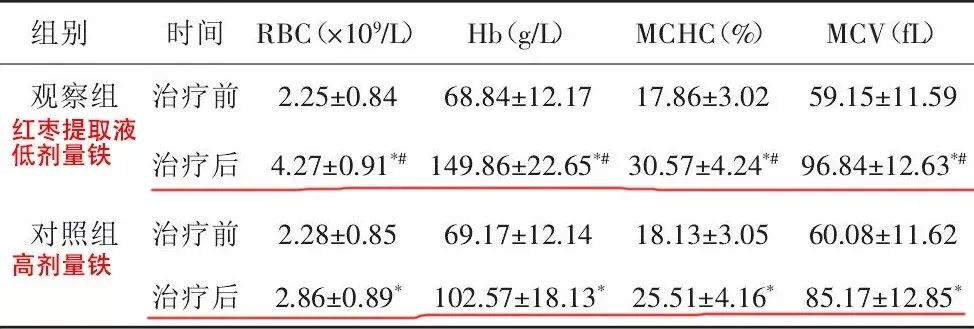
Another study found that jujube extract combined with low-dose iron was more effective in improving pregnancy-related anemia than high-dose iron alone [5].
In studies involving cancer patients, jujube extract was able to elevate hemoglobin levels in leukemia chemotherapy patients within four weeks [6].
Thus, red dates are not ineffective for blood nourishment; they simply have poor iron supplementation effects. Moreover, like other foods, the nutrient content can vary due to factors such as variety and growing conditions, leading to varying blood-nourishing effects.
Additionally, it should be noted that for individuals with iron deficiency anemia, relying solely on red dates is certainly insufficient; appropriate iron supplements must be combined for immediate blood-nourishing effects.
6
Can Ejiao nourish the blood?
In the eyes of many nutrition experts, Ejiao, like red dates, has no blood-nourishing effect because they only focus on iron.
But what if we focus on other types of anemia?
A study involving 72 pregnant women with thalassemia showed that taking 15g of Ejiao daily for four weeks increased hemoglobin levels without changing iron stores [7].
Another study involving 275 women with postpartum anemia indicated that iron deficiency is not the only cause of postpartum anemia, and using Ejiao can improve hemoglobin levels and indicators such as red blood cell volume and distribution width [8].
Furthermore, Ejiao is beneficial for aplastic anemia or chemotherapy-induced anemia [9-12].
Nutritionists often emphasize that Ejiao is made from donkey skin, which is an incomplete protein and thus lacks health value. However, I tell you that the blood-nourishing effect of Ejiao comes precisely from donkey skin; the protein, when broken down, forms short peptide fragments that can activate hematopoietic stem cells and promote blood cell production.
Iron is merely a material for hematopoiesis; there must be someone to direct the work of hematopoietic stem cells. Erythropoietin and testosterone produced by the body are the commanders, and the active components in red dates and Ejiao also play a similar role. This includes turtle shell gelatin and deer antler gelatin, which may have similar “blood-nourishing” effects.
7
Let’s summarize
The causes of anemia vary, and so do the treatment principles.
Aplastic anemia treatment focuses on supportive, symptomatic, and mechanism-targeted therapies, with dietary therapy primarily providing red dates and their extracts or the so-called “inferior proteins” dismissed by some nutritionists, such as Ejiao, turtle shell gelatin, and deer antler gelatin. Certain active components in traditional Chinese medicine can also activate hematopoietic stem cells.
For anemia caused by renal failure, the aforementioned dietary therapies can also be used alongside conventional treatments, and iron supplements can be used if iron stores are clearly low.
Hemolytic anemia requires treatment of the underlying cause while increasing antioxidants like vitamin C and vitamin E to protect red blood cells and extend their lifespan.
For anemia due to insufficient hematopoietic materials, appropriate nutrients should be supplemented: iron for iron deficiency anemia, vitamin B12 and folic acid for megaloblastic anemia, and vitamin B6 for sideroblastic anemia. Additional consumption of red dates and Ejiao can further enhance the effects!

Related Articles (Click to View):
1. Sorry, I was wrong; red dates really can nourish the blood!
2. What’s wrong with donkey skin? This is a treasure; please restore Ejiao’s reputation! Why should the big media’s claims be considered the truth!
References:
1. Hisano, M., Suzuki, R., Sago, H. et al. Vitamin B6 deficiency and anemia in pregnancy. Eur J Clin Nutr 64, 221–223 (2010).2. Irandegani F, Arbabisarjou A, Ghaljaei F, Navidian A, Karajibani M. The Effect of a Date Consumption-Based Nutritional Program on Iron Deficiency Anemia in Primary School Girls Aged 8 to 10 Years Old in Zahedan (Iran). Pediatric Health Med Ther. 2019 Dec 19;10:183-188.3. Chen J, Tsim KWK. A Review of Edible Jujube, the Ziziphus jujuba Fruit: A Heath Food Supplement for Anemia Prevalence. Front Pharmacol. 2020 Nov 26;11:593655.4. Zhang Wenyuan. Clinical Effect Evaluation of Jujube Extract in Improving Pregnancy-Related Thrombocytopenia [J]. Chinese Journal of Maternal and Child Health Research, 2018, 29(11):1444-1447.5. Qiang Jianqin, Guo Yanqing. Clinical Analysis of Low-Dose Iron Combined with Jujube Extract in Treating Pregnancy-Related Anemia in 40 Cases [J]. Clinical Medical Research and Practice, 2018, 3(24):143-144.6. Chinese Journal of Clinical Physicians, September 2016, Volume 10, Issue 18:2715-2718.7. Li Y, He H, Yang L, Li X, Li D, Luo S. Therapeutic effect of Colla corii asinion improving anemia and hemoglobin compositions in pregnant women with thalassemia. Int J Hematol. 2016 Nov;104(5):559-565. Epub 2016 Jul 25.8. Li Yanfang, Ma Danli, Li Daocheng, Du Peiying, Luo Songping. Clinical Efficacy Observation of Compound Ejiao Syrup in Treating Postpartum Anemia Patients [J]. Journal of Guangzhou University of Traditional Chinese Medicine, 2018, 35(04):599-605.9. Liu Weiyan, Ren Rujing, Gao Dengfeng, Gu Jianjun, Liu Guangyuan, Zhang Qingwei, Zhang Yan, Liu Haibin. Research Progress on Compound Ejiao Syrup in Adjuvant Treatment of Malignant Tumors [J]. Journal of Shanghai University of Traditional Chinese Medicine, 2021, 35(01):141-145.10. Zhang Mingyan, Zheng Wenke, Yang Fengwen, Li Yue, Zhang Lishuang, Zhao Hongjie, Ji Zhaocheng, Wang Hui, Zhang Junhua. Systematic Evaluation of the Efficacy and Safety of Compound Ejiao Syrup in Preventing and Treating Bone Marrow Suppression after Cancer Chemotherapy [J]. Tianjin Traditional Chinese Medicine, 2019, 36(05):459-465.11. Cao Leping, Li Xiaoping, Tian Mengying, Cai Jialuo, Liao Fu. Clinical Observation of Ejiao in the Auxiliary Treatment of Chronic Aplastic Anemia [J]. Practical Traditional Chinese Medicine, 2021, 37(04):584-586.12. Huang Jinjun, Zhou Yuehua, Yin Dongfeng. Clinical Research on Ejiao in Treating Cancer-Related Anemia [J]. Asia-Pacific Traditional Medicine, 2018, 14(07):167-169.
Disclaimer:
The content published by this account is for informational sharing only; the views expressed in the article should not be directly used for medical diagnosis or health intervention advice. Please consult your healthcare provider before taking any preventive or therapeutic measures.
More Exciting Content





Are the sisters who like the article 【looking】?